3.4. SAMPLING
4.1.9. 3.4.1. SAMPLE SIZE CALCULATION
We calculated the sample size using EPI_INFO version 3.3 based
on the following:
1. Population size of unmarried young adults in the age group
15-30 years old in the 3 sub-districts under study: 16.944 (data source: KDSS,
see Table 2 ).
2. Expected frequency on level of perceived need towards HIV
premarital examination and of willingness to undergo HIV PCT: 16%. This
expected frequency was drawn from the previous study on VCT establishment where
findings showed that 15.7% of respondents mentioned when one wants to get
married as the main raison for going for VCT 32.
3. Worst acceptable frequency on level of perceived need
towards HIV premarital examination and of willingness to undergo HIV PCT: 10%
(meaning an acceptable margin error of 6%)
4. Confidence level: 95%
5. Computed sample size: 142
Thus a sample size of 142 individuals was targeted. This was
rounded up to 150 unmarried young adult respondents. However
in prevision of eventual drop out from interviews or questionnaire
disqualification due to incompleteness or inconsistency, an extra 20 more
interviews was conducted so that the sample size is fully met.
4.1.10. 3.4.2. SAMPLING METHOD
Non-probability sampling was used. In order to obtain complete
and balanced insight in how knowledge and perceptions towards HIV premarital
examination were distributed in different cultures in males and females, in
rural and urban areas, in educated and illiterate ones, in different religious
and ethnic groups and in different professional categories, all these different
background groups were included in the sample as much as possible in order to
capture a holistic picture.
The main steps in sampling process included the following:
· Purposeful choice of 3 study sub-districts (Kintampo,
Jema Health and New Longoro) and proportionate attribution of quota sample
based on population density of each sub-district.
· Purposeful sampling of key-informants and participants
in IDIs and FGDs.
· Purposive selection of Twelve settlements (towns and
villages) from the 3 sub-districts ( 4 in Kintampo, 4 in Jema Health and 4
in New Longoro) based on population density, geographic location (urban /rural)
and mix of high HIV/AIDS risk (proximity to the highway and prevalence of
stop-over) so that the sample is as much heterogeneous as possible.
· Deduction of proportionate quota sample per
settlement.
· Random selection of 210 compounds out of 3973 (from the
whole total of 19167 in the 3 sub-districts) compounds identified with eligible
respondents from selected settlements, using the computer based data of
Kintampo Demographic Surveillance Survey (KDSS) used in KHRC with STATA command
«draw random sample». Note that the computer ballot system was done
by the KHRC agent, head of field workers in charge of KDSS.
· Selection of respondents: One respondent was selected
per targeted compound.
Any unmarried young adult between 15-30 years old found in any
selected compound was interviewed. In case two or more eligible respondents
were found in the same compound, priority was made on one volunteer who
consented to participate in the interview; otherwise a drawing lot was carried
out to choose only one of respondents who all consented to participate. In case
no respondent was found in a compound, the next selected compounds were
targeted until the full quota sample required was covered.
In order to purposefully equilibrate the sex distribution of
respondents or get a less skewed sex distribution, systematic random selection
of compounds was made from two sex (female and male) sub-sampling computer
based frames drawn from the KDSS which contains data on all the characteristic
of people per registered compound. Thus to each selected compound was assigned
automatically the sex of the respondent to be interviewed.
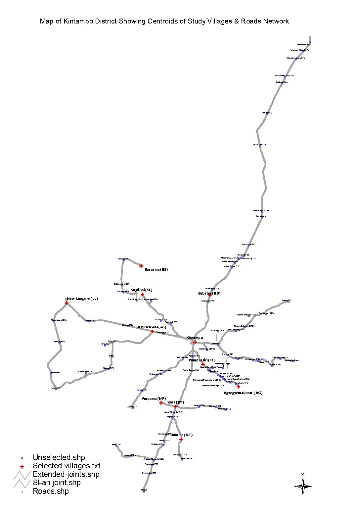
Table 2 describes the selected settlements and their assigned
quota samples. The district map below also describes the geographical situation
of the selected settlements.
|
Table 2: Sampling characteristics of selected towns and
villages per sub-district
|
|
Selected Towns and villages per
Sub-District
|
Town & Village Code
|
Pop. Density
|
Category of settlement
|
HIV Risk Level
|
Number
of RA
|
Population of 15 - 30 years
|
Sample Size*
|
Number
of
Cpd**
|
|
I. KINTAMPO SUB DISTRICT
|
|
1.Kintampo
Town
|
X
|
High
|
Urban
|
High
|
5
|
11066
|
70 (80)
|
100
|
|
2. Agyegye-
makunu
|
AG
|
Low
|
Rural
|
Low
|
1
|
178
|
1 (1)
|
2
|
|
3. Babator City
|
BB
|
High
|
Urban
|
High
|
2
|
1386
|
9 (10)
|
12
|
|
4. Punpuatifi
|
PF
|
Low
|
Rural
|
Low
|
-
|
109
|
1 (1)
|
2
|
|
TOTAL
|
8
|
12739
|
81 (92)
|
116
|
|
II. JEMA SUB DISTRICT
|
|
5. Jema Town
|
JM
|
High
|
Urban
|
High
|
2
|
1542
|
19 (22)
|
26
|
|
6. Nante
|
NN
|
High
|
Rural
|
High
|
1
|
791
|
11 (12)
|
14
|
|
7. Kokuma
|
KK
|
Low
|
Rural
|
Low
|
1
|
312
|
4 (5)
|
6
|
|
8. Ampoma
|
NP
|
Low
|
Rural
|
Low
|
1
|
517
|
7 (8)
|
9
|
|
TOTAL
|
5
|
3162
|
41 (46)
|
53
|
|
III. NEW LONGORO SUB DISTRICT
|
|
9. New Longoro
Town
|
LL
|
High
|
Urban
|
High
|
1
|
402
|
10 (12)
|
14
|
|
10. Asantekwa
|
AS
|
Low
|
Rural
|
Low
|
1
|
283
|
8 (9)
|
11
|
|
11. Busuama
|
BS
|
Low
|
Rural
|
Low
|
1
|
315
|
9 (10)
|
12
|
|
12. Sogliboi
|
SL
|
Low
|
Rural
|
Low
|
-
|
43
|
1 (1)
|
2
|
|
TOTAL
|
3
|
1043
|
28 (32)
|
39
|
|
|
|
|
|
|
OVERALL TOTAL
|
16
|
16944
|
150
(170)
|
210
|
|
Source : Kintampo Health Research Centre (KHRC) demographic
surveillance survey sampling frame and our Field survey, Kintampo (June
2005).
|
|
RA= Research assistants (Interviewers)
|
|
* The number in bracket corresponds to the total sample size
including extra sample units needed for replacement of eventual opt out or
questionnaire disqualification so that an overall sample units of 150 with
consistent and complete questionnaires is met.
|
|
** Number of Compounds selected per town/village in each
sub-District.
|
Figure 0: Map of Kintampo District showing Centroids of study
(villages/Towns) and roads network (Source: KHRC,
June 2005)
| 

